Key Takeaways
- Multi-site marketing breaks at scale because per-location agency models configure the same capabilities repeatedly; treating marketing as an operating model resolves the structural mismatch 1.
- A five-layer stack of strategy, production, distribution, measurement, and governance centralizes goal setting and analytics while leaving community relationships and last-mile adaptation to local sites 2.
- Coordination cost compounds fastest as locations grow, so the decisive criterion is whether capabilities scale linearly per site or stay fixed across the network.
- Sequence the shift over 12 to 18 months by aligning the C-suite first, piloting with co-designed workflows, then retiring per-location retainers in waves 3, 11.
Why marketing structure breaks at the multi-site inflection point
Marketing teams built for one or two sites rarely survive the jump to ten. The team that wrote landing page copy, ran a single Google Ads account, and met weekly with one agency contact suddenly faces a different operating reality: ten brand variants, ten local SEO footprints, ten paid accounts, and a coordination load that grows faster than headcount can absorb.
The break is structural, not effort-based. Research on top-performing healthcare quality departments shows that organizations scaling across sites succeed by centralizing goal setting and decentralizing implementation, with horizontal integration of analytics, ambulatory functions, and shared accountability 2. Marketing operations that ignore that pattern end up with the inverse: decentralized goals, duplicated execution, and no shared analytics layer. Each new location adds a roughly linear increment of agency hours, vendor relationships, and approval cycles.
Deloitte frames the same problem in operating model terms. An operating model is the configuration of internal and external capabilities required to execute on business ambition and customer needs 1. Once a multi-site operator crosses the inflection point, the question stops being who runs marketing and starts being how marketing capabilities are configured. The rest of this article works through that configuration.
Marketing as an operating model, not an org chart
The capability configuration problem
Most marketing reorganizations in multi-site healthcare start with the wrong artifact: a box-and-line diagram. Boxes get redrawn, reports get reassigned, and six months later the same coordination problems return under different titles. The diagram answers who reports to whom. It does not answer what the organization is capable of producing at what cost across how many sites.
Deloitte's working definition is useful here. An operating model is the configuration of internal and external capabilities required to execute on business ambition and meet customer needs, and next-generation models are built to be dynamic, self-learning, and able to adapt to internal priorities and external market shifts 1. Three words in that definition do the work: configuration, capabilities, and external. A multi-site marketing function is rarely one team. It is a configuration of internal staff, agency partners, vendors, freelancers, and increasingly software systems that together produce strategy, content, distribution, and measurement.
Reframing the question changes what gets discussed in a leadership meeting. Instead of debating whether to hire a director of demand generation, growth leaders ask which capabilities the configuration is missing, which are duplicated across sites, and which scale linearly with location count. That is a different conversation, and it produces different decisions.
What clinical quality structures already proved
Healthcare operators do not need to invent the center-led pattern. They already run it on the clinical side.
A peer-reviewed analysis of top-performing healthcare quality departments found that high performers centralize goal setting while decentralizing implementation, integrate analytics and ambulatory functions horizontally across the system, and create shared accountability mechanisms that reach from system leadership to the site level 2. The same study documents the structural drift over the past decade: ambulatory and analytic functions have moved into central quality departments because system-level visibility was impossible without them 2.
The mapping to marketing is direct. Goal setting in marketing means service-line growth targets, brand standards, segmentation frameworks, and channel strategy. Those belong in a central function for the same reason clinical quality goals do: a 40-location dermatology group cannot run 40 different definitions of a qualified lead or 40 incompatible attribution models and still report performance to the board. Analytics belongs centrally for an even simpler reason. GA4, Search Console, ad platform data, and CRM data only produce comparable insight when collected and modeled the same way across every site.
Decentralization still matters, but it applies to a narrower set of activities: community relations, local provider relationships, event partnerships, and the last-mile adaptation of central campaigns to local market language. A behavioral health MSO operating in 14 states cannot run referral relationships from a corporate office. It also cannot afford 14 different brand systems. The center-led model resolves that by separating what travels (standards, analytics, creative systems) from what stays local (relationships, adaptation, on-the-ground execution).
The five-layer capability stack
Strategy layer: goals, segmentation, service-line priorities
The strategy layer answers three questions that should never be answered locally: which service lines get growth investment this year, how the patient audience is segmented across markets, and what the organization will refuse to do. A 22-location orthopedic group with sports medicine, joint replacement, and spine cannot let each site decide its own service-line priority and still produce a coherent paid media plan or a defensible board report.
This is where the center-led pattern documented in top-performing healthcare quality structures applies most directly. High performers centralize goal setting and create shared accountability that reaches from system leadership to the site level 2. For marketing, that means service-line growth targets, the segmentation framework, the qualified-lead definition, and the attribution model live in one place. McKinsey's analysis of healthcare marketing capability building reaches the same conclusion from the executive side: C-suite alignment on marketing priorities is the first of three preconditions for next-generation capability, ahead of capability building itself 11.
The output of the strategy layer is a small, durable artifact: a one-page service-line growth plan with target segments, channel priorities, and the metrics each site will be measured against. Sites do not rewrite it. They execute against it.
Production layer: content, creative, and asset libraries
Production is where per-location agency models bleed cash. Every site commissioning its own service-line landing pages, provider bios, blog content, and ad creative produces duplicated work, inconsistent brand voice, and a content library nobody can find six months later.
The center-led alternative treats production as a shared service feeding a versioned asset library. A core asset gets built once at the service-line level: a knee replacement landing page, a depression treatment explainer, a provider bio template, a paid social creative set. Sites consume those assets with structured local variables, such as provider name, address, insurance accepted, and local proof points. The Forrester organizational design framework calls the underlying discipline competency and capacity mapping, paired with workflow charts that make the production sequence explicit before headcount or vendors are committed 8.
One concrete test separates a working production layer from a broken one. When a new clinical service launches, can the central team ship a complete asset set to every site in one sprint, or does each site queue its own work? The first answer scales. The second does not.
Distribution layer: SEO, paid, and omnichannel governance
Distribution is the layer most operators get wrong by assuming it is a channel problem. It is a governance problem. Local SEO, paid search, paid social, programmatic, email, and SMS each have their own optimization logic, but they share the same patient. The research on omnichannel interaction in health care is explicit: omnichannel is an enterprise capability that demands integrated information systems and cross-channel coordination, not a tactic any single channel owner can execute alone 5. The same review flags data privacy, security, and the operational complexity of managing connected channels in regulated environments as central implementation challenges 5.
For a 40-location dermatology group, that translates into a concrete configuration. Paid search and paid social run from one account structure with location-level ad groups, not 40 separate accounts. Local SEO operates from a centralized listings and review management platform feeding standardized site templates. Email and SMS sequences are built once at the service-line level with local variables injected at send. A central distribution lead owns the cross-channel calendar so that a joint replacement campaign in paid search is not contradicted by a competing dermatology promotion in paid social the same week.
The governance question that distinguishes mature distribution layers from immature ones is simple: who has the authority to pause a channel that is over-spending or under-performing across the network, and how fast can they act? In per-location agency models, that authority sits in 40 different inboxes. In a center-led model, it sits with one role and one dashboard.
Measurement layer: attribution, service-line P&L, executive reporting
Measurement is the layer that decides whether the other four layers survive a budget review. If the CFO cannot see marketing spend tied to service-line revenue at the site level, the entire operating model is one quarterly cycle away from being cut.
The McKinsey priorities for healthcare marketing capability list rigorous measurement as the third precondition, alongside C-suite alignment and methodical capability building through use cases 11. The peer-reviewed quality structure research adds a structural point: top performers centralize analytics horizontally across the system rather than letting each site or service line build its own 2. The reason is mechanical. GA4 properties configured differently across 40 sites produce 40 different versions of a conversion. Ad accounts tagged inconsistently produce attribution that cannot be rolled up. CRM fields defined locally produce a pipeline view the board cannot trust.
A working measurement layer produces three artifacts on a fixed cadence:
- a service-line P&L view that ties marketing spend to attributed revenue,
- a site-level performance scorecard that compares each location against network benchmarks, and
- an executive summary that shows the network trajectory against the strategy layer's targets.
All three come from one data model, not from agency-supplied PDFs reconciled by hand.
Governance layer: compliance, brand integrity, AI oversight
Governance is the layer that makes the other four legally defensible and operationally consistent. It covers HIPAA-aligned review of any patient-facing asset, brand standards enforcement across sites, vendor and platform oversight, and the policies that determine where AI-generated content is allowed, where it requires human sign-off, and where it is prohibited.
The peer-reviewed work on communication and marketing management in patient safety frames marketing governance as a strategic function intersecting clinical and quality domains, not a back-office checkpoint 6. That matters because governance done well becomes a production enabler rather than a bottleneck: a pre-approved asset library, a standing review workflow with defined SLAs, and a clear escalation path for clinical accuracy questions let production move faster, not slower.
The operational question for growth leaders is which decisions require central approval and which can be delegated to site marketers or local agency partners under a published policy. The answer should be written down. When it lives in informal email threads, the network defaults to the slowest possible path on every asset.
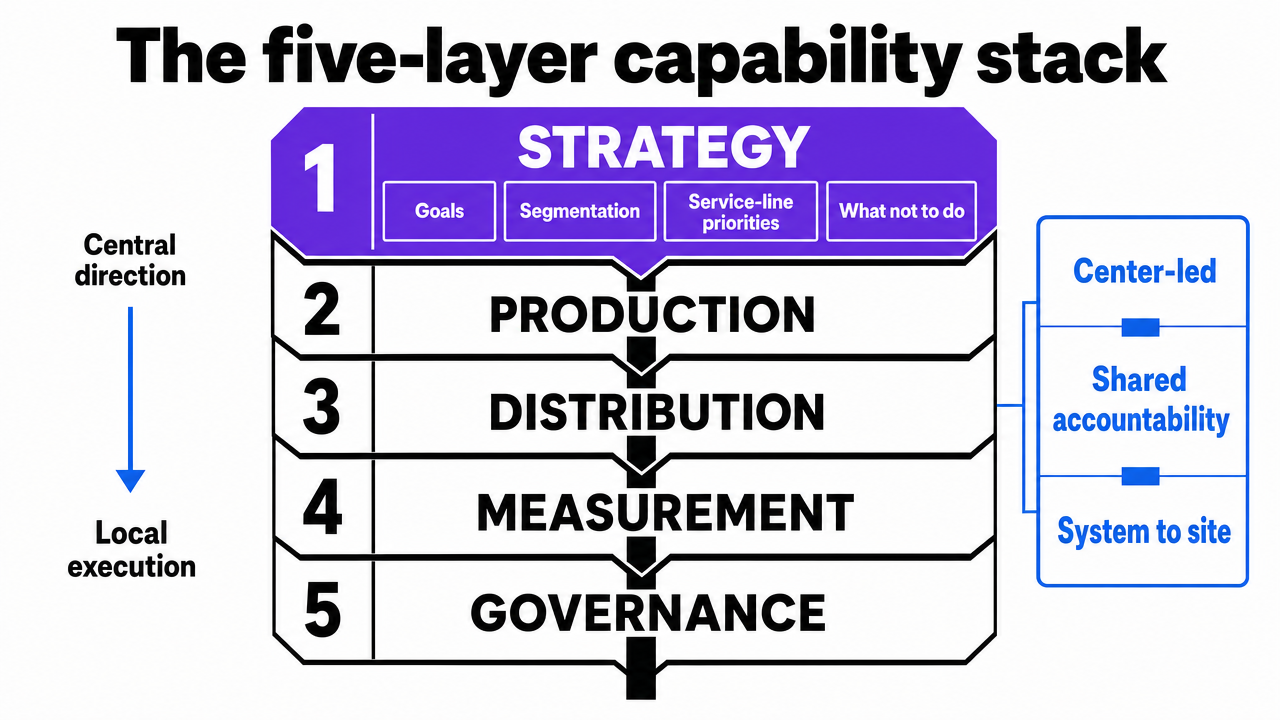 Visualize the five-layer capability stack that structures the entire section, showing how strategy, production, distribution, measurement, and governance relate as a center-led operating model
Visualize the five-layer capability stack that structures the entire section, showing how strategy, production, distribution, measurement, and governance relate as a center-led operating model
Trial full-scale marketing process automation today
Experience hands-on workflow automation and publish live content for your healthcare marketing operations during your trial.
The local-central paradox and how to resolve it
Every multi-site marketing reorganization eventually runs into the same wall. The center publishes a strategy. Sites quietly route around it. Six months later, the network has a polished playbook and 40 versions of execution that contradict it.
The pattern is documented in multi-site healthcare research outside marketing. A qualitative study of hospital-wide patient flow found that frontline staff consistently described tension between local initiatives to improve operations and the absence of a coherent system-wide strategy, with leadership, routine, professional culture, and technology factors intensifying the misalignment under stress 3. The same study concluded that top-down strategies imposed without local co-design tend to backfire, producing overtime and compromised outcomes rather than the intended improvement 3.
The marketing version is recognizable. A local landing page contradicts a central service-line campaign because the site manager wanted faster conversion copy. A regional director keeps a legacy agency on retainer because the central content team missed a deadline last quarter. A site runs a discount promotion the week paid search is bidding on premium positioning for the same service line. None of these are bad-faith choices. They are rational responses to a center that publishes mandates without giving sites a working consumption path.
The resolution is mechanical, not cultural. Each symptom maps to a specific governance mechanism:
- Contradictory landing pages resolve through a versioned asset library with structured local variables, so site adaptation happens inside the system rather than outside it.
- Shadow vendor relationships resolve through a published SLA on central production turnaround paired with a documented exception path.
- Conflicting promotions resolve through a single cross-channel calendar with site-level visibility and a named owner authorized to deconflict.
- Cultural and routine factors, which the patient flow research identified as intensifiers under stress 3, resolve through co-designed workflows where site marketers shape the rules they will execute against, not through edicts from a corporate office.
The diagnostic test is whether the center makes local execution easier or harder. If sites route around it, the answer is already known.
If a multi-site operator manages 10 or more locations: the consolidation economics
This section narrows the audience. The capability stack applies to operators of any size, but the economics flip hard somewhere between five and ten locations. Past that threshold, per-location agency retainers stop being a manageable line item and start dictating the shape of the marketing function.
The mechanism is configuration, not effort. Deloitte's operating model frame treats marketing as the configuration of internal and external capabilities required to execute on ambition and customer needs 1. Per-location retainers configure the same capability N times. Account-level execution configures it once and applies it across N sites.
The table below compares cost drivers under each model. No dollar figures are used; the variable is N, the number of locations. Scaling behavior is labeled linear (O(N)), sub-linear, or fixed.
| Cost driver | Per-location retainer model | Account-level execution model | Scaling as N grows |
|---|---|---|---|
| Strategy hours | N strategy calls, N plans | One network plan, site variants | Linear vs. fixed |
| Content production | Assets rebuilt per site | Service-line assets, local variables | Linear vs. sub-linear |
| SEO audits | N standalone audits | One audit framework, site rollups | Linear vs. sub-linear |
| Paid media management | N accounts, N managers | One account, location ad groups | Linear vs. sub-linear |
| Reporting | N PDFs, hand-reconciled | One data model, site scorecards | Linear vs. fixed |
| Coordination meetings | N standing calls | One network cadence | Linear vs. fixed |
The cost driver to watch is coordination. It is the line item operators rarely price and the one that compounds fastest. At 40 sites, a weekly 30-minute agency check-in per location consumes 20 hours of internal time before any work product changes hands. That hour count is fixed in the account-level model regardless of whether N is 10 or 100.
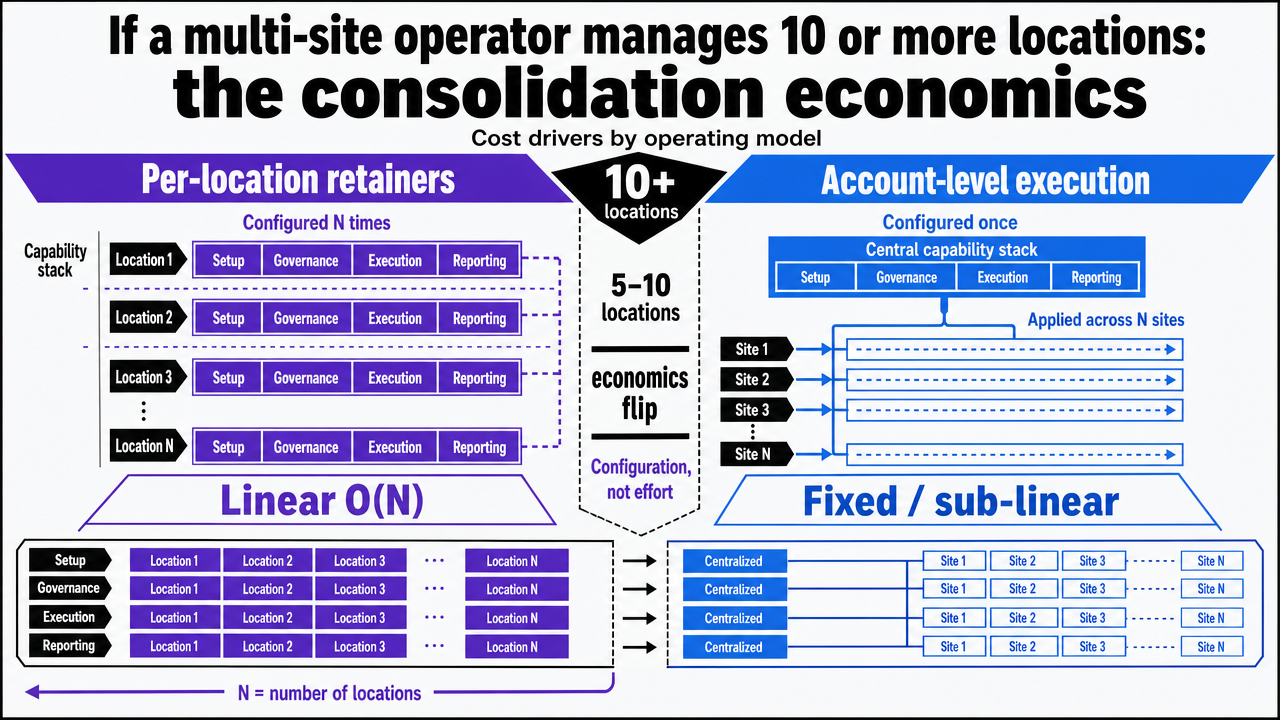 Reinforce the comparison table by visualizing how cost drivers scale linearly under per-location retainers versus staying fixed or sub-linear under account-level execution
Reinforce the comparison table by visualizing how cost drivers scale linearly under per-location retainers versus staying fixed or sub-linear under account-level execution
Aligning the C-suite before redesigning the team
Restructuring marketing before the C-suite agrees on what marketing is for produces an expensive reorganization that solves nothing. McKinsey's analysis of next-generation healthcare marketing capability lists C-suite alignment as the first of three preconditions, ahead of capability building and rigorous measurement 11. The order matters. A growth leader who redesigns the team without that alignment ends up defending the new structure quarter after quarter against executives who still treat marketing as a referral-support cost center.
The alignment conversation is narrow and concrete.
- The CFO needs to see how marketing spend will tie to service-line revenue once the new model is in place.
- The COO needs to know which decisions move from sites to the center and which stay local.
- The Chief Medical Officer needs a written policy on clinical accuracy review and AI-generated content.
- The CEO needs a one-page view of how the configuration changes the cost curve as locations grow.
None of these are abstract. Each maps to an artifact the operating model must produce.
Skipping this step is what turns a center-led redesign into the local-central paradox documented in multi-site healthcare research, where top-down strategies without executive co-ownership get routed around by frontline operators 3. Alignment first, structure second.
See How Leading Healthcare Operators Streamline Marketing Team Processes
Connect with experts to benchmark your multi-site marketing workflows and discover scalable process models that reduce manual coordination as you expand.
Sequencing the transition: 12 to 18 months without breaking local performance
The transition itself is where most center-led redesigns fail. Sites cannot go dark on patient acquisition while corporate builds a new operating model, and a 40-location group cannot rip out 40 agency relationships in a single quarter without losing revenue.
The sequence that protects local performance runs in three phases.
- Months 1 through 4 build the strategy and measurement layers first: one service-line growth plan, one analytics data model, one qualified-lead definition, and a site-level scorecard running in parallel with existing agency reporting. Nothing changes for local execution yet. The point is to make the network legible before restructuring it. McKinsey's preconditions, C-suite alignment and rigorous measurement, anchor this phase 11.
- Months 5 through 10 build the production and distribution layers under a pilot cohort, typically four to six sites representing the mix of service lines and market types. Central content, consolidated paid accounts, and a unified listings platform run alongside legacy vendors for the cohort only. Pilot sites co-design the workflows they will execute, which is the mechanism the patient flow research identifies as the antidote to top-down strategies that get routed around 3.
- Months 11 through 18 roll the validated configuration across remaining sites in waves, retiring per-location retainers as each wave clears its performance gate. The governance layer hardens last, once the workflows it governs are actually running.
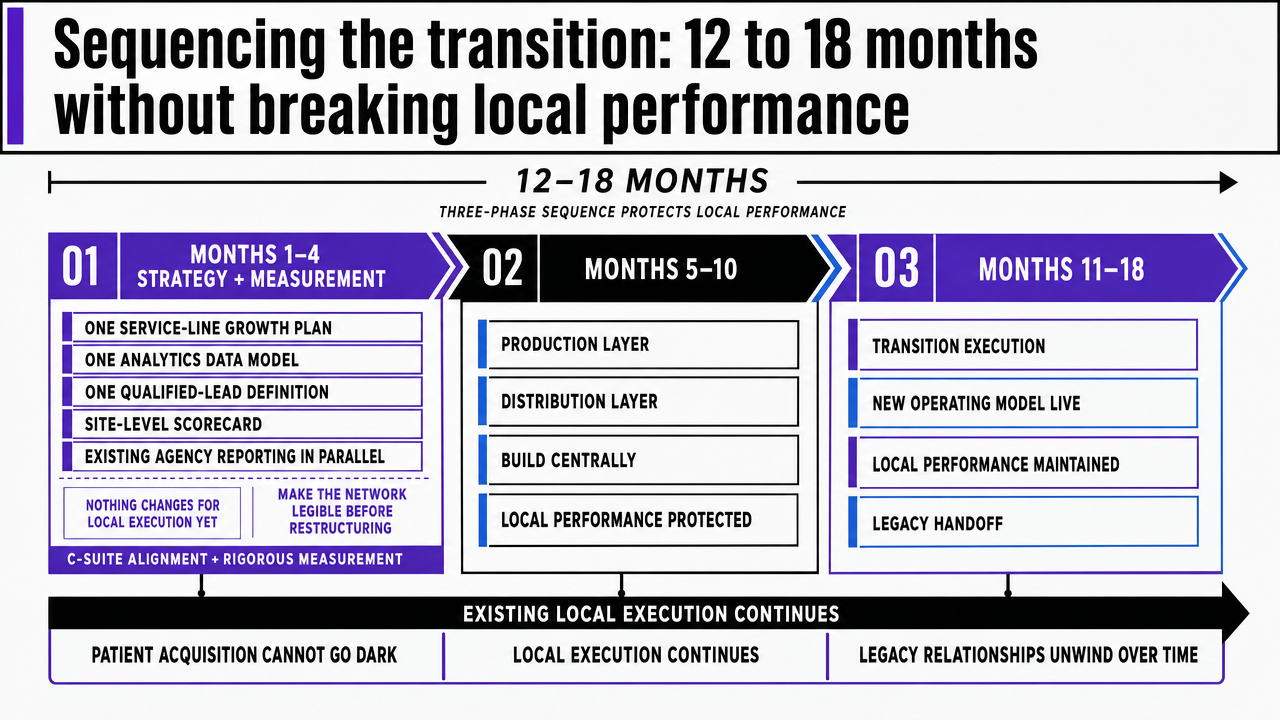 Visualize the three-phase 12-18 month transition timeline cited in the section, showing what builds in each phase and how legacy operations run in parallel
Visualize the three-phase 12-18 month transition timeline cited in the section, showing what builds in each phase and how legacy operations run in parallel
What changes when AI capabilities sit inside the stack
AI does not replace the five-layer stack. It collapses the cost curve of running it.
Production is the layer where the shift shows up first. Service-line landing pages, provider bios, paid social variants, and local SEO content that once required N agency briefs now generate from one structured input, with human review concentrated on clinical accuracy and brand fit rather than first drafts. Measurement compresses next: cross-account data normalization, anomaly detection, and site-level scorecards run continuously instead of monthly. Distribution governance gets faster when a single system can flag a paid channel pacing off target across 40 locations in hours, not weeks 5.
The governance question is where most operators stall. Physicians are already comfortable working with digital tools alongside clinical workflows 4, but marketing leaders still need a written policy: which AI outputs ship after machine review, which require human sign-off, and which never auto-publish. Without that policy, AI capability becomes another shadow vendor relationship the center cannot see.
Closing: what a working operating model produces
A working marketing operating model produces three things a per-location agency stack cannot.
- The cost curve bends as locations multiply, because capabilities are configured once and consumed N times rather than rebuilt at every site 1.
- The network becomes legible, because one analytics layer, one qualified-lead definition, and one service-line P&L view replace 40 reconciliations 2.
- Local execution gets faster, because sites consume central assets through structured workflows instead of routing around mandates they had no part in designing 3.
That is the operating model multi-site healthcare growth leaders need. Vectoron was built to run it.
Frequently Asked Questions
References
- 1.Designing an Operating Model for Changing Market Needs.
- 2.A Roadmap to Excellence: Insights From Quality Structures of Top Performing Health Care Organizations.
- 3.Bottom-up perspectives on hospital-wide patient flow – a multi-site qualitative study of solutions to organisational paradoxes.
- 4.AMA: Physicians propelling health care's digital transformation.
- 5.An Overview of Omnichannel Interaction in Health Care Services.
- 6.Communication and Marketing Management in Patient Safety.
- 7.The Connection of Marketing and Healthcare Management.
- 8.Healthcare Spotlight: Marketing Organizational Design.
- 9.The Strategy That Will Fix Health Care.
- 10.The Value Journey: Multihospital Systems.
- 11.Marketing in healthcare: Improving the consumer experience.
- 12.The impact of marketing strategies in healthcare systems.