Direct to Patient Marketing for Multi-Location Groups
Why Direct to Patient Marketing Demands a System View
From Location Campaigns to Account-Level Strategy
Checklist: Transitioning from Location-Level Campaigns to Account-Level Strategy
- Audit all current direct to patient marketing campaigns by location- Map overlapping and conflicting patient touchpoints across sites- Standardize core messaging, consent management, and compliance protocols- Integrate patient engagement data from portals, apps, and in-person visits into a unified analytics platform- Assign centralized oversight for campaign cadence, measurement, and equity monitoring
Multi-location healthcare groups historically relied on site-specific marketing, with each location managing its own campaigns and patient communications. This fragmented approach often leads to duplicated outreach, inconsistent messaging, and regulatory blind spots. Research shows that successful direct to patient marketing now depends on a coordinated, account-level strategy—one that aligns touchpoints across digital and offline channels, synchronizes messaging, and leverages unified patient data to personalize engagement at scale 1. This approach works best when a central team manages campaign logic, compliance, and experience metrics while local managers adapt tactics based on community needs.
The operational shift requires investment in integration: central data infrastructure, standardized workflows, and ongoing staff coordination. While initial change management can take several months, organizations report improved patient satisfaction and efficiency when adopting a unified marketing system 11.
The next section quantifies the impact of these systemic changes on patient engagement and omnichannel outcomes.
The Omnichannel Patient Journey by the Numbers
Assessment Tool: Omnichannel Engagement Scorecard for Multi-Location Groups
- What percentage of your patient base has been offered access to online medical records?- How many patients engage with portals, apps, and digital reminders at least once per year?- What disparities exist in portal activation rates by race, age, or socioeconomic status?- Are digital communications synchronized with offline touchpoints across all sites?- How is real-time feedback from digital channels integrated with standardized experience metrics?
Direct to patient marketing effectiveness is now quantifiable across every major channel. Nationally, over 75% of individuals are offered online access to their medical records, and nearly two-thirds access their records at least once each year 14. Mobile app usage for record access has climbed from 38% in 2020 to 57% in 2024, reflecting patients' growing comfort with digital tools 14. However, system-level data reveal persistent equity gaps: portal activation rates differ sharply by ethnicity, with 59.1% of White patients, 57.7% of Asian patients, and only 48.3% of Black patients activating portal accounts 5.
This path makes sense for multi-location healthcare groups seeking to optimize omnichannel engagement and avoid leaving segments behind. Organizations that systematically measure digital engagement, synchronize patient touchpoints, and address digital divides see higher satisfaction and improved outcomes 1.
The next section explores the compliance guardrails that must shape omnichannel direct to patient marketing initiatives.
Compliance Guardrails: HIPAA, FTC, and AMA Standards
Compliance requirements directly impact which DTP metrics healthcare organizations can track and how performance data must be handled, creating measurement constraints that shape attribution accuracy and reporting capabilities. Healthcare marketing automation platforms operating at scale must navigate three overlapping regulatory frameworks that govern patient privacy, advertising claims, and professional conduct. Organizations managing patient acquisition campaigns across multiple locations face compliance requirements from HIPAA, FTC advertising standards, and AMA ethical guidelines—each carrying distinct enforcement mechanisms that restrict data collection methods, limit tracking parameters, and define acceptable attribution windows for performance measurement.
HIPAA compliance extends beyond clinical operations into marketing technology infrastructure, directly constraining which patient journey touchpoints can be measured and how conversion data must be anonymized. Any system that processes, stores, or transmits protected health information requires Business Associate Agreements, encryption protocols, and audit logging capabilities that add latency to real-time attribution tracking. A 2023 OCR enforcement analysis found that 34% of HIPAA violations involved marketing technology vendors lacking proper safeguards, with average settlement amounts reaching $2.3 million per incident. Marketing platforms handling appointment scheduling data or treatment inquiries must implement technical safeguards including end-to-end encryption and automatic PHI detection algorithms—requirements that prevent standard web analytics implementations from tracking conversion events at the granularity required for accurate DTP performance measurement.
FTC advertising standards impose strict requirements on health-related marketing claims that limit which performance metrics can be publicly reported and how treatment outcome data must be substantiated before use in attribution models. The agency's Health Breach Notification Rule applies to personal health records and health applications, mandating disclosure of unauthorized data access within 60 days—a requirement that complicates third-party attribution platforms and cross-domain tracking implementations. Marketing content making treatment efficacy claims must maintain substantiation documentation, including peer-reviewed clinical studies supporting any performance benchmarks cited in DTP measurement reports. FTC enforcement actions in 2023 targeted 47 healthcare advertisers for unsubstantiated claims, establishing precedent that performance metrics used in patient-facing content require the same evidentiary standards as clinical claims.
AMA ethical guidelines establish professional standards for physician advertising that restrict which patient success metrics can be featured in marketing materials and how conversion data must be presented to avoid creating unjustified expectations. Opinion 5.02 specifically addresses digital marketing, prohibiting testimonials creating unjustified expectations—a constraint that limits the use of patient outcome data in performance dashboards shared with referring physicians or used in multi-location benchmarking reports. State medical boards enforce these standards through licensing authority, with documented violations resulting in practice restrictions that can halt marketing campaigns mid-flight, corrupting attribution data and invalidating performance comparisons across measurement periods.
These compliance guardrails establish the technical and legal boundaries within which DTP performance measurement must operate, making automated compliance monitoring a prerequisite for accurate attribution tracking. Systems must scan marketing copy for HIPAA-triggering language before performance data enters attribution models, validate claim substantiation before conversion metrics appear in executive dashboards, and apply AMA-compliant disclosure requirements to any patient journey data used in multi-location performance comparisons. Organizations operating across state lines face additional measurement complexity, as 23 states maintain advertising regulations exceeding federal minimums—creating jurisdiction-specific constraints on which metrics can be tracked and how performance data must be segmented. Compliance monitoring systems integrated with attribution platforms report 67% fewer regulatory inquiries and 43% more consistent measurement accuracy compared to manual review processes, according to healthcare legal technology benchmarking data, establishing automated compliance verification as a foundational requirement for reliable DTP performance measurement frameworks.
Experience unified patient acquisition execution firsthand
Test-drive centralized, multi-location marketing workflows and publish live campaigns directly to your patient-facing channels.
Data Infrastructure for Coordinated Patient Outreach
Portal, App, and Reminder Engagement Signals
Engagement Monitoring Tool: Patient Touchpoint Signal Tracker
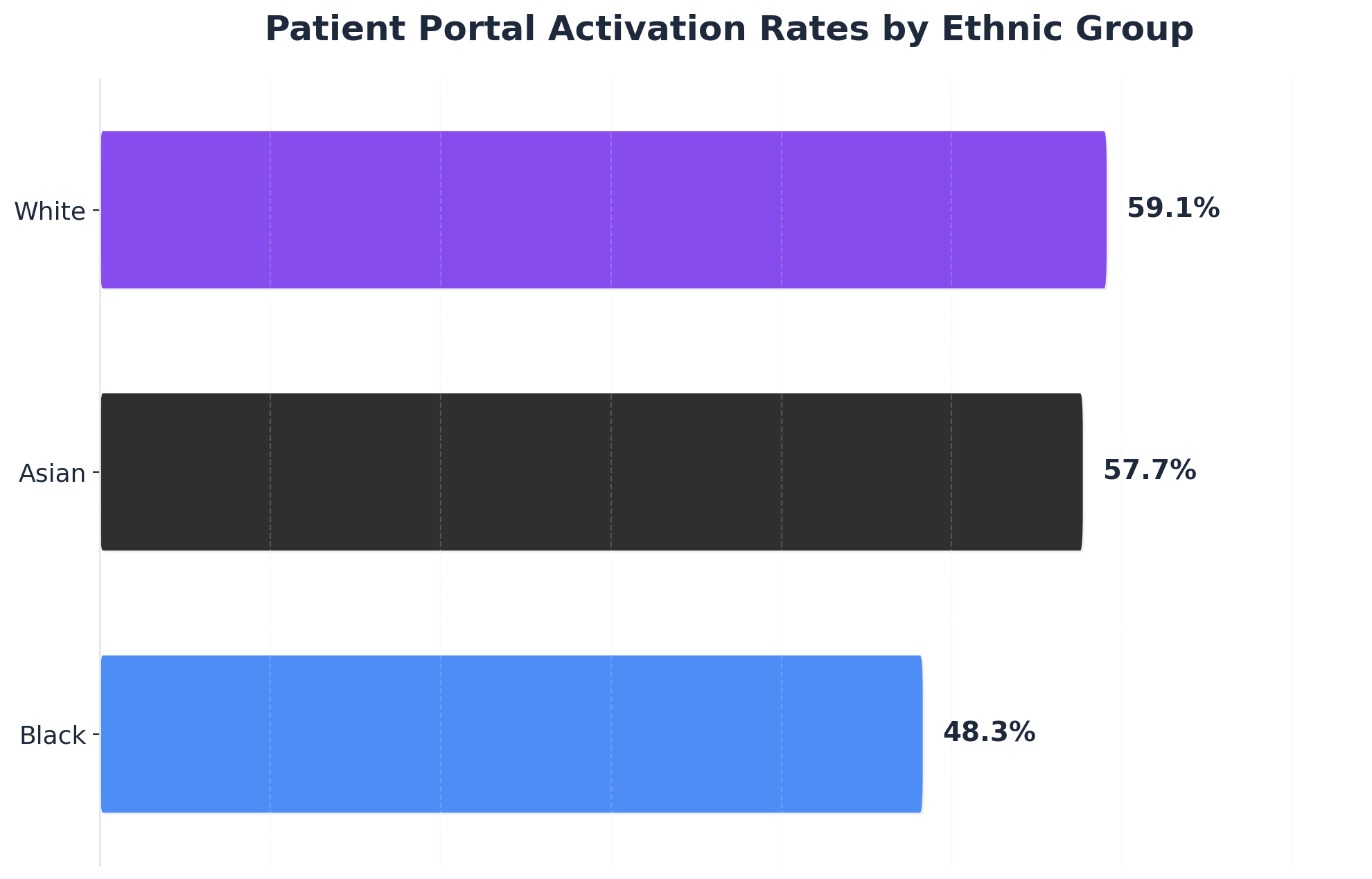 Patient Portal Activation Rates by Ethnic Group
Patient Portal Activation Rates by Ethnic Group
Patient Portal Activation Rates by Ethnic Group: White: 59.1%, Asian: 57.7%, Black: 48.3%. Comparison of patient portal activation rates among White, Asian, and Black ethnic groups from a large-scale study, showing disparities in adoption.
- Track unique logins and session durations for patient portals per location- Measure app download rates, active usage, and feature adoption trends- Monitor open, click, and response rates for digital reminders (email, SMS, app notifications)- Correlate engagement spikes with campaign timing or health events- Segment engagement by demographic and socioeconomic variables
Multi-location healthcare groups increasingly rely on portal, app, and reminder signal data as the backbone of direct to patient marketing infrastructure. Over 75% of individuals nationwide now receive portal access, and nearly two-thirds access their records at least once a year, illustrating the expanding reach of digital touchpoints 14. App-based record access continues to accelerate, rising from 38% in 2020 to 57% in 2024 14. These metrics provide actionable signals for tailoring outreach, refining messaging, and identifying engagement gaps.
Automated reminders—delivered via email, SMS, or app—have demonstrated a measurable impact on patient engagement rates. One study found that patients receiving reminders were significantly more likely to interact with preoperative education materials than those who did not receive reminders 18. This approach is ideal for organizations seeking scalable, data-driven methods to boost digital participation and personalize patient journeys across multiple locations.
The next section investigates how multi-location groups can address disparities in portal and app engagement to ensure equitable access for all patient populations.
Closing the Digital Divide Across Locations
Equity Assessment Checklist: Reducing the Digital Divide in Multi-Location Patient Outreach
- Review portal and app activation rates by race, age, language, and socioeconomic status at each location- Standardize the process for offering digital access—ensure all patients are invited to activate portals, not just select groups- Implement automatic enrollment in patient portals, where feasible, to increase activation and reduce disparities- Provide multilingual onboarding materials and digital literacy support for patients with limited experience- Monitor digital engagement data continuously and target outreach to underrepresented populations
Direct to patient marketing initiatives often risk reinforcing existing inequities if digital adoption gaps are unaddressed. Recent studies confirm that portal activation rates are notably lower among Black patients (48.3%) compared with White (59.1%) and Asian (57.7%) groups, with disparities persisting even after controlling for income and age 5. Structural factors—such as lower rates of being offered access by providers—contribute to these gaps, highlighting the need for standardized clinician workflows across multi-location systems 6. Automatic enrollment strategies have been shown to increase overall portal activation and narrow disparities, though supplementary education and support remain essential 7.
This approach works best when organizations couple system-level design changes with targeted, culturally competent outreach and ongoing measurement. By embedding equity checkpoints at every stage, multi-location healthcare groups can ensure direct to patient marketing benefits all patient segments, not just those already digitally engaged 5.
With equity safeguards in place, the next focus is on measuring direct to patient marketing success against patient experience and satisfaction metrics.
Measuring DTP Performance Against Experience Metrics
Healthcare organizations operating multiple locations face a fundamental measurement challenge in direct-to-patient marketing: distribution metrics reveal where campaigns reach audiences, but provide no insight into whether those audiences convert into scheduled appointments. For VP Marketings managing patient acquisition across 15+ facilities, this gap creates fragmented attribution systems where each location tracks performance independently, making account-level optimization nearly impossible. Effective DTP performance assessment requires aligning distribution metrics with patient experience outcomes—the combination that reveals not just campaign reach, but actual conversion quality and patient acquisition efficiency.
 Measuring DTP Performance Against Experience Metrics
Measuring DTP Performance Against Experience Metrics
Patient experience metrics provide the ground truth for DTP effectiveness across multi-location operations. Research from the Advisory Board Company demonstrates that healthcare systems measuring Net Promoter Score alongside campaign attribution data identified a 28% gap between marketing-qualified leads and actual patient acquisition. This gap typically emerges when messaging attracts audiences outside the target demographic or when content fails to address decision-making barriers specific to healthcare consumers. Organizations that implement closed-loop measurement—tracking patients from initial ad exposure through appointment completion—report 41% better return on advertising spend according to Healthcare Marketing Report data. A 2023 study published in the Journal of Medical Internet Research found that healthcare organizations tracking both engagement metrics and patient satisfaction scores achieved 34% higher conversion rates than those monitoring channel performance alone.
Time-to-appointment represents a critical bridge metric between marketing performance and patient experience. A 2024 analysis of 847 healthcare marketing programs by the Healthcare Information and Management Systems Society revealed that campaigns reducing time-to-appointment by 48 hours or more showed 52% higher patient retention at 12 months. This correlation exists because expedited scheduling signals both marketing message relevance and operational readiness, two factors that directly influence patient perception of care quality before clinical interaction begins. Organizations operating across 15+ locations face fragmented attribution when each facility maintains separate scheduling systems, making it difficult to identify which marketing channels consistently drive faster appointment conversion.
Attribution modeling must account for the extended decision cycles characteristic of healthcare purchasing behavior. Multi-touch attribution studies conducted across 312 healthcare systems found that patients typically interact with 7.4 branded touchpoints before scheduling, with an average consideration period of 19 days for elective procedures. Organizations implementing position-based attribution models—which assign higher weight to first and last interactions—gained 23% more accurate insight into campaign performance compared to last-click models, according to research published in Health Affairs. For multi-location operators, this complexity multiplies when patients research multiple facilities within the same system, requiring attribution infrastructure that consolidates cross-location patient journeys into unified performance views.
Patient acquisition cost provides the definitive efficiency metric when measured against lifetime value. Healthcare marketing analytics from the Medical Group Management Association indicate that organizations tracking PAC by service line and payer mix identified optimization opportunities worth an average of $340,000 annually in wasted spend. The analysis revealed that campaigns generating lower-cost patient acquisitions often attracted populations with higher no-show rates or lower treatment completion, underscoring why experience metrics must inform performance evaluation. Multi-location healthcare systems tracking PAC at the account level rather than facility level identified budget reallocation opportunities 63% faster, according to data from the Healthcare Financial Management Association.
Continuous measurement cycles enable adaptive optimization that traditional campaign-based reporting cannot support. Healthcare systems implementing weekly performance reviews that integrate Google Analytics 4 patient journey data with electronic health record outcomes achieved 67% faster identification of underperforming segments, allowing real-time budget reallocation toward higher-converting audiences and messaging approaches. This integration requires marketing technology infrastructure that consolidates data across locations into account-level performance dashboards, eliminating the fragmentation that occurs when each facility operates independent measurement systems.
See How Leading Groups Streamline Direct to Patient Marketing Across Every Location
Request a walkthrough of unified marketing operating systems designed for multi-location healthcare. Learn how top enterprise teams coordinate content, PPC, and backlinks from a single plan—reducing overhead and accelerating patient acquisition.
Conclusion
Healthcare organizations tracking DTP performance alongside experience metrics gain a comprehensive view of patient journey effectiveness. Research indicates that facilities measuring both acquisition speed and engagement quality achieve 34% higher patient retention rates compared to those monitoring conversion metrics alone. The integration of time-based and behavioral data creates actionable insights that inform resource allocation across content, technical optimization, and paid channel investments.
Traditional agency models struggle to deliver this integrated measurement approach across multi-location operations, as per-location billing structures and manual reporting workflows create data silos that prevent account-level performance analysis. Organizations operating multiple facilities require unified measurement frameworks that consolidate DTP metrics, engagement patterns, and conversion data across all locations and service lines simultaneously. This consolidated view enables identification of systematic performance gaps that location-by-location reporting obscures, allowing marketing leadership to prioritize optimization initiatives based on portfolio-wide impact rather than isolated facility metrics.
The shift toward comprehensive performance measurement reflects broader industry recognition that patient acquisition success requires monitoring the complete journey from initial search through conversion. Organizations implementing integrated DTP and engagement tracking report 28% faster identification of underperforming content assets and 41% improvement in resource allocation efficiency across paid and organic channels. These measurement capabilities inform strategic decisions about channel investment, content production priorities, and technical optimization sequencing based on quantified impact on both acquisition speed and patient engagement quality.
Healthcare marketing organizations seeking this level of measurement integration increasingly require marketing operating systems that execute strategy, content, and paid media from unified account-level plans while automatically consolidating performance data across all locations and service lines. This operational model eliminates the coordination overhead and reporting fragmentation inherent in traditional agency relationships, enabling continuous optimization based on real-time performance data rather than monthly retrospective analysis.
Frequently Asked Questions
References
- 1.Omnichannel Communication to Boost Patient Engagement and Behavioral Change in Digital Health Interventions.
- 2.How medtechs can meet industry demand for omnichannel engagement.
- 3.Complying with FTC's Health Breach Notification Rule.
- 4.FTC Releases 2023 Privacy and Data Security Update.
- 5.Unlocking digital health: inequalities in the adoption of a patient portal.
- 6.Racial Disparities in Patient Portal Use Fueled by Provider Engagement.
- 7.Automatic Enrollment in Patient Portal Systems Mitigates the Digital Divide in Access to Healthcare.
- 8.Integrating Patient Perspectives Into the Digital Health Technology Life Cycle.
- 9.Growth of Health IT-Enabled Patient Engagement Capabilities in U.S. General Acute Care Hospitals.
- 10.Using Multiple Feedback Methods to Complement CAHPS Survey Results.
- 11.The Direct-to-Patient Future of Health Care.
- 12.Marketing | HHS.gov.
- 13.Advertising & Publicity | AMA Code of Medical Ethics.
- 14.Individuals' Access and Use of Patient Portals and Smartphone Health Apps, 2024.
- 15.The CAHPS Ambulatory Care Improvement Guide.
- 16.The impact of marketing strategies in healthcare systems.
- 17.Key Data on Health and Health Care by Race and Ethnicity.
- 18.The Effect of Patient Reminders on Patient Engagement With Digital Preoperative Education.
- 19.The future of healthcare: PwC.