Key Takeaways
- Patient conversion stalls when the website, location pages, and portal are treated as separate properties; treating them as one continuous conversion surface exposes recoverable drop-offs at each handoff.
- Readiness signals like motivation, privacy comfort, and prior digital experience predict conversion more reliably than demographics, and they can be addressed through on-page copy, form length, and consent framing 2.
- Usability defects—errors, workarounds, missed actions, and buried information—are the real drivers behind low form completion and high call volume, and aesthetic redesigns rarely fix them 1, 6.
- Multi-location operators should shift work from per-page creative to template-level fixes, continuous postdeployment monitoring, and measurement tied to confirmed EHR appointments rather than form submissions 12.
Why patient acquisition stalls at the portfolio level
Most healthcare growth programs lose patients not because marketing fails, but because the website, location pages, and patient portal lack a unified conversion strategy. A prospective patient might search for a symptom, land on a service page, abandon an intake form, and then call a front desk unaware of the digital handoff failure. This issue, multiplied across numerous locations and EHR-connected portals, creates a structural impediment to schedule fill rates.
The common response is a website redesign, but evidence suggests this is often ineffective. AHRQ's lifecycle framework emphasizes usability and conversion as continuous operational practices, requiring ongoing monitoring rather than one-off projects 12. The Health IT Playbook similarly advocates for optimization as workflow improvement, not periodic cosmetic updates 4.
Three factors exacerbate this problem:
- First, templated location pages mean a usability flaw on one page affects all.
- Second, portals often reside on separate domains with distinct analytics, obscuring handoff drop-offs.
- Third, agency coordination costs increase linearly with the number of locations, while conversion improvements do not, leading to diminishing returns for each marginal gain.
The solution is not more creative design, but a continuous measurement loop that treats every location page and portal handoff as a single conversion surface, constantly optimizing it.
Readiness, not demographics, predicts whether a visitor converts
Demographic targeting by age, ZIP code, or income is less effective for predicting conversion than often assumed by growth teams. Research using the AHRQ-funded PRE-HIT instrument found that patients who enrolled in a portal had an average PRE-HIT score of 73.8, compared to 57.9 for those who declined 2. This difference correlated with motivation, privacy comfort, prior internet experience, and perceived relevance of online health information, rather than demographic categories.
Operationally, this means a 58-year-old with a high readiness profile is more likely to convert than a 28-year-old with low motivation or privacy concerns. Location pages and intake forms that segment by age or insurance type are relying on weak signals. The crucial signals—desire for self-service, trust in digital data handling, and prior online task experience—are behavioral and emerge during the session.
For portfolio operators, this reframes audience targeting. First, the readiness gap is detectable through analytics by observing:
- time spent on FAQ and privacy content,
- scroll depth on service explanations,
- repeat visits before form attempts,
- and hesitation on contact forms.
These behaviors proxy for motivation and trust. Second, low-readiness visitors don't need different campaigns; they need a tailored on-page experience. A qualitative review found that empowerment and personalization drive digital health tool adoption, while digital literacy and privacy concerns are primary barriers 14. These barriers can be addressed through copy, form length, and consent framing, not just media buying.
For multi-location operators, the practical approach is to view each location page as a readiness filter, not just a billboard. A page that addresses privacy concerns before asking for a phone number, explains post-submission steps, and offers a phone fallback for low-readiness visitors will convert a broader segment of traffic. This recovers potential abandonments through on-page work, which is cost-effective once templated, rather than through increased ad spend.
The PRE-HIT data also resolves a common debate within growth teams. When a location underperforms, the usual explanations are media mix or local competition. Readiness data suggests a third, cheaper-to-test explanation: the page itself is inadvertently filtering out motivated visitors due to unmeasured friction.
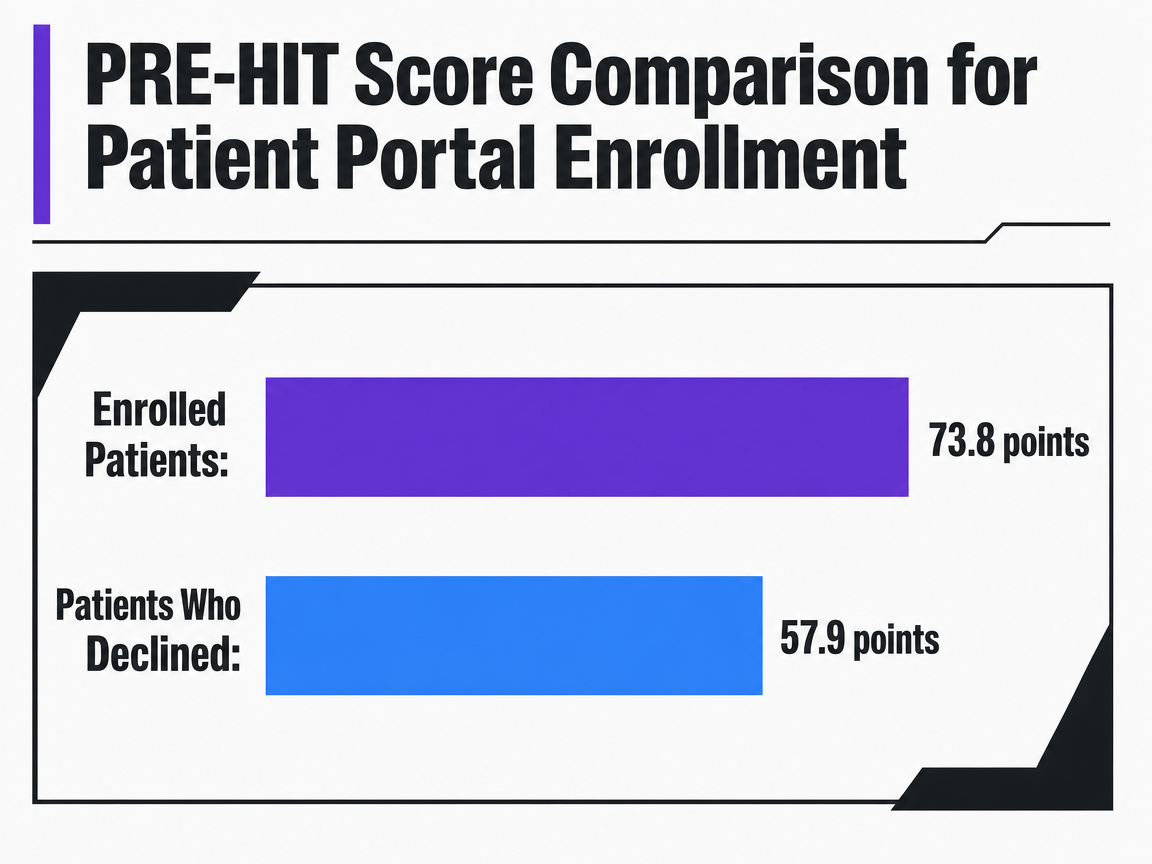 PRE-HIT Score Comparison for Patient Portal Enrollment
PRE-HIT Score Comparison for Patient Portal Enrollment
Compares the average Patient Readiness to Engage in Health Information Technology (PRE-HIT) score between patients who enrolled in a patient portal and those who declined.
Usability failures are conversion failures in disguise
NIST's human factors guide for high-risk healthcare settings identifies four common failure indicators: outright errors, workarounds, missed actions, and critical information buried behind multiple clicks 1. While written for EHR interfaces, this taxonomy applies directly to public-facing websites. For example:
- A visitor who mistypes a date on an intake form without inline correction commits an error.
- One who abandons a form to call the front desk creates a workaround.
- Closing a tab before submitting a request is a missed action.
- Inability to find scheduling information without navigating through multiple service descriptions indicates buried critical information.
Growth teams often misinterpret these as low form-completion rates, high inbound call volumes, flat schedule fills, or "underperforming" service lines, rather than usability defects. The underlying problem is the same; only the reporting layer obscures it.
NIST's guidance recommends that important information be accessible with one click or hover, and navigation burden minimized for faster task completion 5. On a location page, this means a scheduling action visible above the fold, insurance and accepted-provider details answered proactively, and forms that validate input in real-time rather than rejecting submissions post-facto.
The debate between aesthetics and usability is settled by portal-adoption literature. A study on design simplicity found that visual appeal only boosted portal use when combined with actual ease of use; attractive but confusing layouts did not improve adoption 6. For website teams, this implies that a redesign improving a location page's appearance without addressing form logic, scheduling paths, or field validation will not impact conversion rates. The investment yields a softer brand impression but the same abandonment rate.
AHRQ's broader framework links design quality to workflow and information transfer, not just surface presentation 11. For multi-location operators, this shifts the audit focus from outdated page aesthetics to identifying pages that generate measurable errors, workarounds, missed actions, and buried critical information. Each failure leaves a digital trace:
- Errors appear as field-level retries in form analytics;
- workarounds as spikes in inbound calls from visitors who started digital tasks;
- missed actions as session recordings where a scheduling button was viewed but not clicked;
- and buried information as scroll depth and on-page searches for terms like "appointment," "insurance," or "hours."
These four signals are vital signs for conversion optimization. They are observable on every location page using existing instrumentation and pinpoint areas for improvement before any design work begins. A growth team conducting this audit across templated location pages typically finds recurring defects, allowing a single, propagated fix to recover conversion across the entire footprint without per-location creative effort.
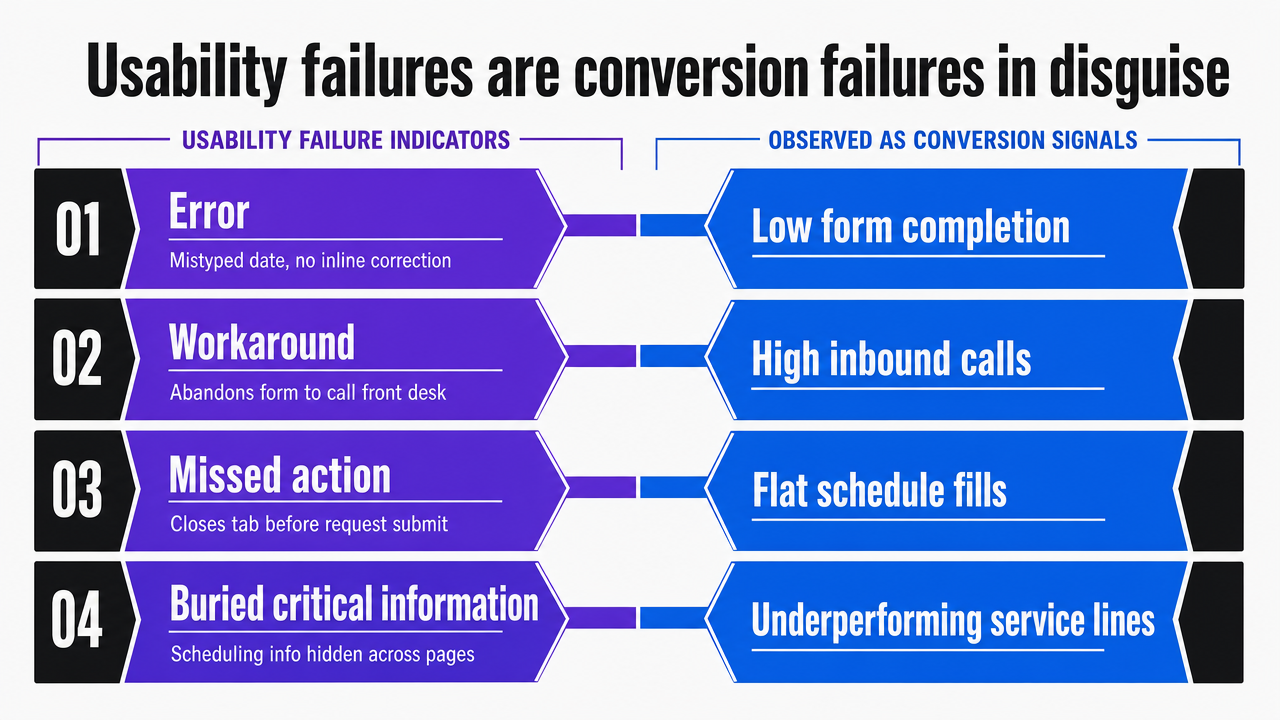 Visualize the four NIST-cited usability failure indicators and how each maps to an observable conversion signal, directly supporting the section's framework
Visualize the four NIST-cited usability failure indicators and how each maps to an observable conversion signal, directly supporting the section's framework
Test Conversion Improvements on Live Healthcare Sites
Experience data-backed optimization and publish real campaigns to evaluate measurable conversion gains in your own environment.
The website, the location page, and the portal are one conversion surface
The patient portal transitioned from a back-office utility to a critical patient touchpoint between 2014 and 2022. ONC data shows that the percentage of individuals offered and accessing their online medical records more than doubled during this period, making portal access a standard expectation 13. For operators, this means the portal handoff is no longer the end of the patient journey but a high-volume conversion event, often unmeasured as such by growth teams.
The distinction between a marketing site and a portal is an internal organizational artifact; patients perceive a continuous task. A visitor who requests an appointment on a service page and is then redirected to a separate domain to create portal credentials views this as one continuous process. If the portal has separate analytics, a drop-off during credential creation might still be counted as a marketing conversion, leading to a discrepancy with the actual schedule fill rate weeks later.
CMS's national quality strategy addresses this as a digital access issue, promoting standards-based Patient Access APIs to bridge system gaps 3. For growth teams, this implies a need for a single instrumentation layer across the website, location page, and portal to track visitors through credential creation, first portal login, and first scheduled visit. Without this, it's impossible to determine if conversion lift comes from an improved intake form or merely shifts abandonment downstream.
AHRQ frames this as a workflow and information transfer challenge, not just page-level UX 11. The website initiates the appointment request, the portal handles identity verification, insurance details, and consent, and the EHR receives the booking. Each handoff is a potential point where a motivated visitor becomes a missed conversion, and these handoffs are often managed by different teams within healthcare organizations. This fragmented ownership is a primary reason for persistent conversion leaks, as data does not flow across organizational silos.
Treating these three properties as a single conversion surface changes measurement priorities. Form-completion rate is no longer the primary metric. Instead, the key metric becomes the percentage of visitors who arrive on a location page and achieve a confirmed appointment in the EHR, with drop-off attributed at each handoff point. This figure is typically lower than marketing reports indicate, and this gap represents recoverable conversion opportunities.
Designing for the patients most likely to drop off
While the instinct is to optimize for the most likely converter, growth mathematics suggests focusing on the marginal conversion: the motivated visitor who hesitated and left. This group disproportionately includes individuals with lower digital literacy, active privacy concerns, or chronic conditions that heighten the perceived risk of errors. A systematic review of online health information-seeking behavior found that age, income, employment, and education significantly influence digital channel engagement, and careless digital-first design choices can exacerbate these disparities 15.
Counterintuitively, designing for the more challenging cohort does not negatively impact conversion for the easier one. A patient portal study involving adults with diabetes, including those with limited health literacy, reported above-average usability ratings across the entire cohort and sustained anticipated use 8. Plain language, fewer fields, explicit next-step descriptions, and a clear phone fallback do not hinder high-readiness visitors; they recover lower-readiness ones.
The same review that identified digital literacy and privacy as barriers also highlighted empowerment and personalization as motivators 14. These two factors create tension in form design: personalization often requires more fields, while privacy advocates for fewer. The resolution lies in sequencing: ask for essential booking information first, and defer details needed for treatment. A location page demanding insurance details, referral source, and reason-for-visit before confirming an appointment prioritizes back-office convenience at the expense of visitors most likely to abandon.
AHRQ's review of interventions for vulnerable populations points to a frequently overlooked failure pattern: access without activation 7. Visitors reach a page, see a form, but never start it. This non-attempt is often miscategorized as low traffic quality in analytics, rather than a design defect. Treating it as a design flaw—due to buried scheduling, unclear privacy posture, or a missing phone fallback—transforms an equity issue into a conversion lever, rather than a mere compliance footnote.
A/B testing as postdeployment monitoring, not a quarterly project
Many growth teams approach A/B testing like brand refreshes: a scheduled cycle, a fixed list of variants, a readout, and a long gap until the next round. AHRQ's lifecycle framework for health IT views experimentation differently. Usability testing, postdeployment monitoring, and lifecycle evaluation are continuous practices throughout a property's lifespan, not time-bound projects 12. The website is the product, and the testing program is its operational mechanism.
Precedent for structured experimentation in healthcare already exists. A pilot study on a clinical trial recruitment website used A/B variants for design and information presentation, proving effective for optimizing recruitment materials and campaigns 17. For portfolio operators, the key takeaway is not just that A/B testing works, but that it is justifiable for sensitive healthcare journeys when variants focus on information clarity, form structure, and task paths, rather than manipulating clinical decisions.
Operating A/B testing as continuous monitoring rather than a project changes three aspects:
- First, the measurement unit shifts from "test won or lost" to tracking error rates, workaround rates, and missed-action rates over time across the location-page template. A 0.3-point lift from a single test is less significant than the same lift applied across 40 templated location pages.
- Second, the cadence becomes continuous, not quarterly. Methodological guidelines for health-related digital assessment describe web analytics as an embedded, continuous measurement layer that enhances usability and conversion, not a periodic audit 9.
- Third, governance adapts. Variants affecting privacy posture, consent language, or clinical content follow a slower review track. Variants related to field order, button placement, validation timing, and copy clarity move on a fast track. Treating all variants at the same pace often stalls healthcare experimentation programs.
This continuous loop also addresses the attribution gap at the portal handoff. When variants are evaluated against confirmed appointments in the EHR, rather than just form submissions on the marketing site, the testing program begins to reward changes that genuinely fill schedules, instead of those that merely shift abandonment downstream.
See How Scalable Conversion Optimization Reduces Per-Site Cost Across Complex Healthcare Networks
Request a demonstration of data-driven workflows that automate multi-site website conversion improvements, eliminate manual coordination, and deliver consistent results for enterprise-scale healthcare and agency teams.
If you manage multiple locations: the coordination-cost view
Why per-location optimization breaks at scale
For operators managing numerous locations, conversion optimization evolves from a design challenge into a coordination problem. While a single-site team can afford bespoke work for every page, a 40-location operator cannot. This reality often becomes apparent only after multiple quarterly redesigns fail to produce measurable improvements in schedule fill rates.
The breakdown is mechanical. Location pages are typically templated, meaning a single defect—such as a buried scheduling CTA, a form rejecting valid insurance entries, or a privacy paragraph loading below the fold—replicates across the entire footprint. Fixing it once requires modifying every page, every analytics view, and navigating multiple approval queues. The AHRQ Health IT Playbook frames this as workflow integration, not creative work, emphasizing continuous operational optimization over redesign cycles 4. This framing is crucial because it reassigns ownership of the lift: creative ownership scales linearly with locations, but workflow ownership does not.
A second compounding factor is the handoff between the marketing site, location page, and patient portal. Each handoff often involves a different system owner, analytics tag, and vendor. AHRQ's design-for-safety work highlights information transfer between systems as a recurring failure point 11. For a portfolio operator, this translates to a measurement gap: conversion is recorded on the site, but abandonment occurs at the portal, and no single dashboard provides a holistic view. This leak persists because the organizational chart and the data layer are misaligned.
A coordination-cost comparison: traditional model vs portfolio model
The economic shift becomes evident when coordination costs are quantified using variables operators already track: number of locations, service lines, monthly coordination hours per location, and approval handoffs per change. Methodological guidelines for health-related digital assessment argue that web analytics function as an embedded, continuous measurement layer, not a periodic audit 9. This logic extends to deployment: changes implemented across the entire portfolio in one pass are significantly more cost-effective than per-location changes.
The table below compares coordination costs, assuming consistent creative and content quality, using only operator-tracked variables and one published price point.
| Variable | Traditional per-location agency model | Portfolio-level optimization model |
|---|---|---|
| Unit of work | Per location, per service line | Per template, propagated across footprint |
| Coordination handoffs per change | Brief, draft, review, revise, deploy — repeated per location | Brief, draft, review, deploy once to template |
| Cycle time for a single conversion fix | Weeks per location, sequenced | Days, applied across all locations in one pass |
| Measurement layer | Per-location reports, manually reconciled | Single instrumentation layer across site, location pages, and portal handoff |
| Cost behavior as locations grow | Scales linearly with locations and service lines | Fixed account-level engagement; published trial at $599/mo (Vectoron) |
| Portal handoff visibility | Usually uncounted; lives outside marketing analytics | Tracked as a conversion event inside the same loop |
This comparison illustrates that the cost curves diverge. A 5-location operator might not feel the impact, but a 40-location operator incurs these costs every cycle, and a 200-location operator pays twice: once in agency hours and again in lost conversions because fixes never reach the page.
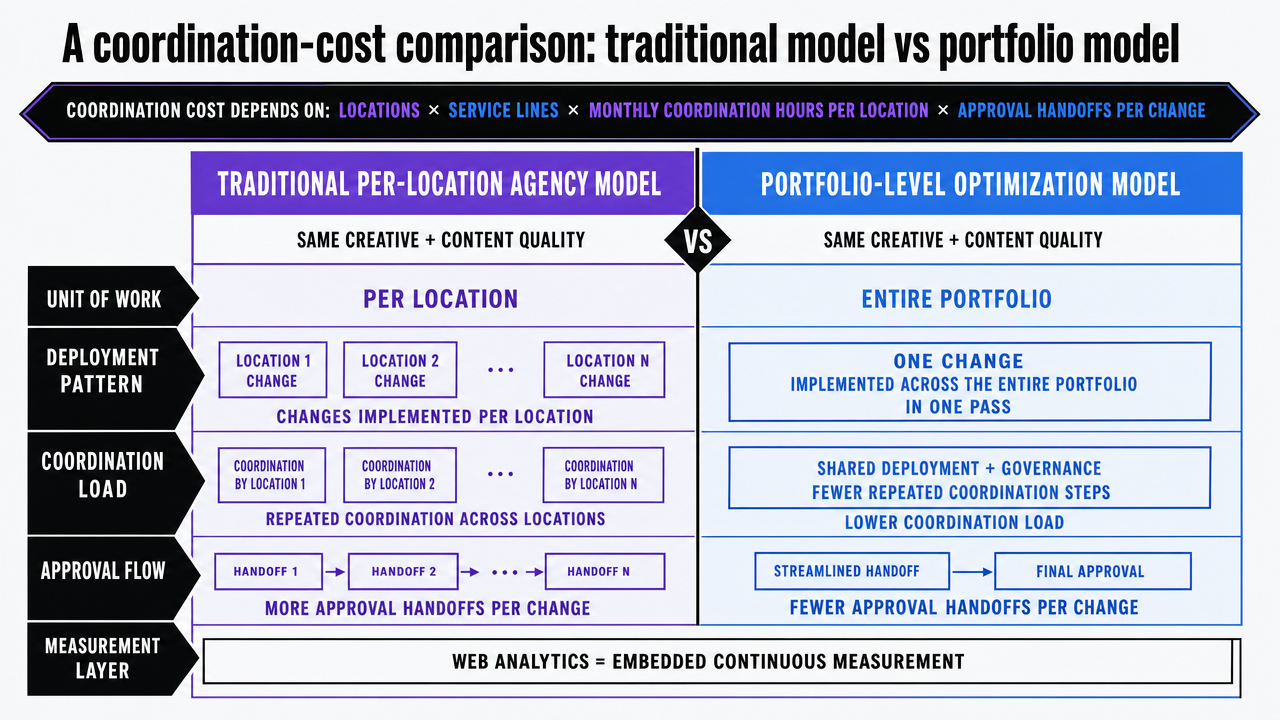 Render the section's comparison table as a clean side-by-side infographic so readers can scan the operating-model differences quickly
Render the section's comparison table as a clean side-by-side infographic so readers can scan the operating-model differences quickly
Operating the measurement loop without doubling headcount
The primary barrier for most healthcare growth teams to implement continuous optimization is not analytical capacity, but staffing. A measurement loop that monitors form-field errors, portal handoff drop-offs, scroll depth on privacy content, and confirmed appointments in the EHR requires regular review and decision-making. Staffing this role per location would make the program financially unsustainable.
Methodological work on health-related digital assessment offers an alternative: web analytics as an embedded measurement layer that continuously augments usability and conversion, rather than a periodic audit 9. "Embedded" means instrumentation, variant queues, and deployment paths are integrated into a single operating rhythm, not confined to quarterly agency cycles or separate analyst spreadsheets.
Three operational choices enable this loop without additional headcount:
- First, the unit of work is the template, not the individual page. A defect found on one location page leads to a single fix propagated across the entire footprint, mirroring AHRQ's logic for system-level workflow optimization 4.
- Second, the variant queue is prioritized by review weight. Changes to field order, validation timing, copy clarity, and CTA placement move quickly. Anything involving consent language, privacy posture, or clinical content follows a slower clinical-review path. Mixing these paces often stalls internal programs.
- Third, the reporting layer culminates in confirmed appointments in the EHR, not just form submissions. AHRQ's lifecycle framework for usability evaluation treats postdeployment monitoring as an ongoing operational mode, not a project phase 12, and the only metric that justifies this approach is one directly tied to schedule fill.
For operators seeking to implement this without establishing an internal CRO function, the practical step is to utilize a system that manages instrumentation, variant production, and deployment at the account level. Vectoron offers a two-week trial at $599/mo for teams exploring this operating model.
Frequently Asked Questions
References
- 1.A Human Factors Guide to Enhance EHR Usability of Critical User Interactions when Supporting Pediatric Patient Care.
- 2.Patient Readiness to Use Internet Health Resources.
- 3.Quality in Motion: CMS National Quality Strategy.
- 4.Electronic Health Records - Health IT Playbook.
- 5.A Human Factors Guide to Enhance EHR Usability of Critical User Interactions when Supporting Pediatric Patient Care.
- 6.Design simplicity influences patient portal use: the role of aesthetic appeal and usability.
- 7.Interventions to increase patient portal use in vulnerable populations.
- 8.The My Diabetes Care Patient Portal Intervention: Usability and Preliminary Effects.
- 9.Methodological Guidelines for Systematic Assessments of Health-related Websites and Apps.
- 10.Certified EHR Technology.
- 11.Institute for the Design of Environments Aligned for Patient Safety.
- 12.Electronic Health Record Usability.
- 13.Individuals' Access and Use of Patient Portals and Smartphone Health Apps, 2022.
- 14.Patients' Perspectives on Digital Health Tools: A Qualitative Review.
- 15.Online Health Information Seeking Behavior: A Systematic Review.
- 16.A Cross-Sectional Survey of Online Health Information Seeking Behavior among Undergraduate Students.
- 17.A/B Design Testing of a Clinical Trial Recruitment Website: A Pilot Study.