Key Takeaways
- Multi-site marketing breaks around 25 locations when retainer models built on weekly calls and per-location briefs collapse into coordination overhead instead of patient acquisition output 9.
- Conventional RFPs reward deck polish over execution, so vendors who invest in pitch theater outscore those whose operations actually hold together past location 25.
- Score vendors on six criteria that predict scaled performance: compliance-aware measurement, location-level data integration, account-level execution, healthcare KPI reporting, unit economics discipline, and team plus AI capability.
- Allocate 100 RFP points by failure mode, weighting execution capacity at 25 and measurement at 20, then add three or four hard deal-breakers to prevent chemistry-driven ties 3.
- Per-location retainers scale linearly while coordination cost grows faster, so account-level programs and AI-driven production protect blended CAC against the sourced $155–$610 range 4.
- Match operating model to footprint: centralized agencies fit 5–15 sites, modular stacks suit 25–75 with strong internal ops, and account-level execution is required past roughly 50 locations.
- Lock the rubric into contract terms — written CAC and CAC:LTV triggers, account-level pricing, operator data ownership, 72-hour reporting SLAs, and termination rights for missed performance 5.
The 25-Location Breakpoint That Breaks Most Agency Models
Multi-site healthcare marketing fails at a predictable threshold. Around 25 locations, the operating model that worked for a single clinic or a tight regional cluster stops scaling: campaigns ship late, locations execute inconsistently, and account managers spend more time coordinating than producing 9.
The breakpoint is structural, not cultural. A retainer agency built around weekly status calls and per-location creative briefs does not become more efficient at 40 locations or 80 locations. It becomes more expensive per patient acquired, slower to publish, and more dependent on the institutional memory of whichever account lead happens to still be on the team. That is also where vendor risk concentrates: 44% of practices that switch core vendors cite an unresponsive partner as the primary reason, a pattern that maps directly onto agency churn at scale 1.
The selection question for a VP of Marketing running 10, 50, or 200 sites is therefore not which agency wins the pitch. It is which operating model survives past the 25-location threshold without collapsing into coordination overhead. That reframing changes what belongs in the RFP. Strategic deck quality, retainer price, and account team chemistry move down the priority list. Account-level execution architecture, location-level data integration, compliance-aware measurement, and shipping cadence move to the top — because those are the variables that actually correlate with patient acquisition outcomes once the location count crosses the threshold where manual coordination breaks.
Why Conventional Agency Selection Fails Multi-Site Operators
The standard healthcare RFP rewards the wrong skills. It privileges deck design, brand storytelling, and the polish of a finalist presentation — capabilities that signal pitch quality but say almost nothing about whether a vendor can publish 400 location pages, run 60 paid search accounts, and keep tracking compliant for 18 consecutive months without something breaking.
That mismatch shows up in the evaluation categories most multi-site operators inherit from procurement. A representative healthcare RFP weighting — strategic approach, creative capability, execution excellence, KPI measurement, total cost, and credibility — distributes points evenly across criteria of very unequal predictive value 8. Strategic approach and creative capability are easy to score from a deck. Execution excellence at scale is not. The result is that vendors who invest in pre-sale theater outscore vendors who invest in post-sale operations, even though only the second group can hold the contract together past location 25 9.
Three habits compound the problem. First, lowest-cost bias: procurement often defaults to retainer price as a tiebreaker, when sourced guidance on RFP scoring is explicit that lowest cost rarely wins on long-term value 3. Second, generic must-haves: when every requirement is marked critical, nothing differentiates vendors, and weighted scoring collapses into a tie 1. Third, undefined measurement: agencies are asked to report KPIs without the RFP specifying which decision types those KPIs are meant to inform, so reporting drifts toward whatever is easiest to produce rather than what the operator needs to allocate budget 10.
A selection process built for multi-site reality scores vendors against the failure modes that actually appear at 25, 75, and 200 locations — not against the artifacts produced during the eight weeks of the pitch.
Test Unified Medical Marketing Across All Sites
Experience multi-site campaign execution and results measurement with full platform access for seven days, risk-free.
Six Evaluation Criteria That Predict Multi-Site Performance
Compliance-Aware Measurement Architecture
Measurement is the first criterion because it is the one most agencies fail quietly. Healthcare's privacy constraints rule out the cookie-based, user-level attribution that most agencies built their reporting stacks around. An agency that cannot articulate which measurement approach it uses for which decision type will default to whatever its dashboard tool happens to support — usually last-click attribution that overstates branded search and undercounts everything upstream.
The diligence question is specific. Agencies should be able to map measurement technique to decision type: marketing mix modeling for budget allocation across service lines, geo-based incrementality tests for channel-level decisions, and conversion lift studies for campaign-level questions 10. If a vendor proposes a single attribution model for every decision, that is a tell. The model is not wrong because it is simple; it is wrong because the operator cannot use it to defend budget shifts to a CFO.
Score this criterion against four artifacts: a written measurement plan tied to specific business decisions, a documented HIPAA-compliant tracking architecture, a method for handling consent-mode and signal loss, and named examples of incrementality or holdout tests run for prior healthcare clients. Vendors who cannot produce all four are reporting, not measuring.
Location-Level Data Integration
Data integration determines whether reporting reflects what is actually happening in each market or only what is easy to aggregate. A 50-location operator needs GA4, Search Console, Google Ads, and call-tracking data joined at the location level, with conversion definitions that reconcile to PMS or EHR booking records. Most agencies stop at the platform-level dashboard.
The capability test is whether the vendor can show a single location's full funnel — impressions, clicks, calls, form fills, booked appointments, kept appointments, revenue — within a working environment, not a slide. Agencies that rely on monthly exports and manual joins will fall behind as the location count grows; the work scales linearly while the margin does not.
Two follow-up questions separate operators from order-takers. First, how does the agency handle locations with different EHR or scheduling systems, which is common in roll-up structures. Second, what is the latency between a booking event and its appearance in marketing reporting. Anything above 72 hours forces budget decisions to lag market signal by a full week, which is expensive at scale.
Account-Level Execution Capacity
Execution capacity is the criterion that breaks at 25 locations and the one most underweighted in conventional RFPs. The question is not whether the agency can produce a campaign for one site. It is whether the operating model can ship 50 location pages, 30 paid search builds, and a quarterly content refresh across the portfolio without a status meeting for every change 9.
The signal to look for is whether the vendor plans, prices, and executes at the account level or the location level. Per-location retainers, per-location creative briefs, and per-location reporting cadences are leading indicators of the failure mode. Account-level operating models — one strategy plan, one production pipeline, one approval queue, with location-specific outputs derived from a shared spec — survive scaling because the marginal cost of adding a location is small.
Score this criterion on three concrete questions. How many discrete deliverables did the agency ship across all clients in the last quarter, normalized by headcount. What is the average cycle time from brief to publication for a location page or paid search build. And how does the agency handle a request to launch a new market in 30 days. Vendors who answer these in days and units, not adjectives, are the ones whose operations actually scale.
Performance Reporting Against Healthcare KPIs
Reporting is where vendor accountability becomes contractual. Agencies should report against the established healthcare KPI categories operators already use to manage the business — patient acquisition, conversion, retention, revenue per patient, and channel-specific efficiency — not against a custom marketing-only dashboard that does not reconcile to operational reality 5.
The minimum reporting spec for a multi-site contract includes location-level CAC by channel, MQL-to-consult and consult-to-treatment conversion rates, kept-appointment rates by acquisition source, and 12-month patient revenue cohorts. Agencies that report only on impressions, clicks, and form fills are reporting on inputs; the operator needs outputs.
Two diligence checks separate strong reporting from theatrical reporting. First, can the dashboard drill from portfolio total to a single location and a single provider within three clicks. Second, does the agency proactively surface which locations are underperforming the portfolio mean and what the recommended action is, or does it wait for the operator to ask. Reporting that cannot drive action does not justify its production cost at any location count.
Unit Economics Discipline
Unit economics discipline separates agencies that understand healthcare growth from agencies that sell marketing services. The benchmarks are sourced and stable: patient acquisition costs range from roughly $155 to $610 depending on specialty, lifetime value typically falls between $10,000 and $20,000 per patient relationship, and a CAC:LTV ratio at or below 1:3 signals healthy economics 4.
An agency that cannot quote these ranges, locate the operator's portfolio inside them, and propose channel mix against them is not running a healthcare practice. It is running a generalist practice with a healthcare logo on the website. The diligence question is whether the vendor commits, in writing, to a target blended CAC by service line and a quarterly review against the 1:3 threshold — and what happens contractually if the ratio slips.
This is also the criterion where lowest-cost bidding most often misleads. A retainer that is 20% cheaper but produces a blended CAC 40% above benchmark is not cheaper; it is more expensive per acquired patient, with the gap compounding monthly. Sourced RFP guidance is direct: lowest cost rarely wins on long-term value, and clear ROI commitments matter more than headline pricing 3. The contract should price the relationship in CAC and CAC:LTV terms, not just monthly fees.
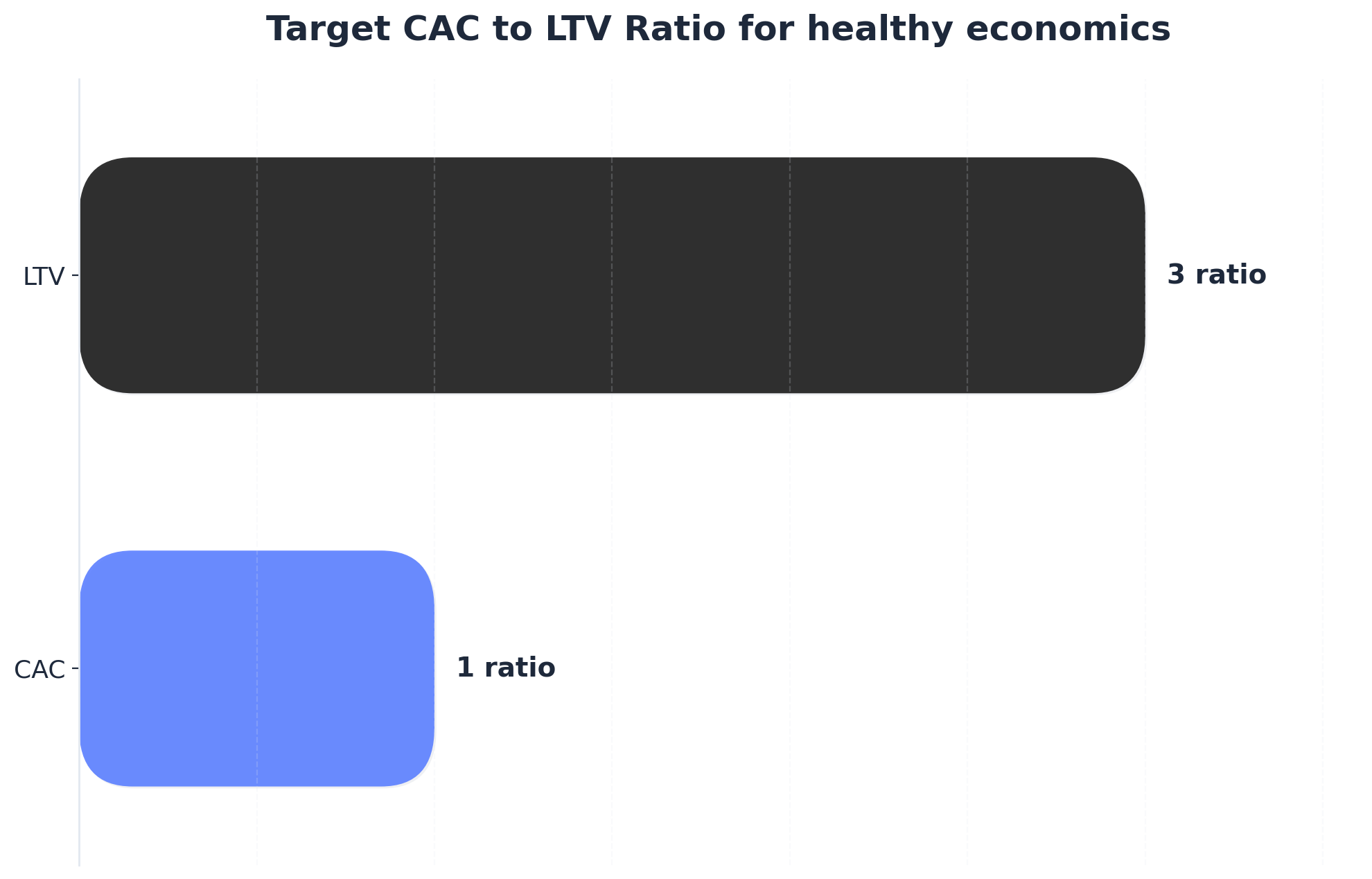 Target CAC to LTV Ratio for healthy economics
Target CAC to LTV Ratio for healthy economics
Target CAC to LTV Ratio for healthy economics: CAC: 1ratio, LTV: 3ratio. A 1:3 ratio of Customer Acquisition Cost to Lifetime Value is a common benchmark for healthy marketing economics in healthcare.
Team Depth and AI Execution Capability
Team depth and AI execution belong in the same criterion because both answer the same underlying question: can the vendor produce the volume of work a multi-site portfolio requires without coordination drag. Healthcare marketing in 2025–2026 assumes baseline capability in AI-powered personalization, privacy-first measurement, local SEO at scale, omnichannel journey design, and short-form video 6. Agencies still selling those as premium add-ons are behind the market.
Team depth is partially observable through credentials. Certified, experienced marketing managers command roughly $34,000 more in annual compensation than uncertified entry-level peers, which is a useful proxy for whether the agency is staffing senior practitioners on the account or rotating juniors through it 7. Ask for the named team, their certifications, and the percentage of their time contractually allocated to the account.
AI capability is the harder evaluation because the term is overused. The diligence questions are operational. Where in the production workflow is AI generating, optimizing, or routing work, and what is the human review step. What is the documented quality control process for medical accuracy. And does the AI deployment translate into measurable cost-per-acquisition reduction — sourced benchmarks point to roughly 30% CAC improvement when AI-driven marketing is implemented well, which gives operators a number to hold the agency to rather than a slogan to nod at 4.
A Weighted Scoring Rubric for the RFP
Weighted scoring is the mechanism that prevents pitch theater from outranking operational substance. The rubric below allocates 100 points across the six criteria established earlier, with weights set against multi-site failure modes rather than presentation polish. Two principles drive the allocation: criteria that predict performance past 25 locations carry more weight than criteria that signal pitch quality, and any criterion can include a deal-breaker threshold that disqualifies a vendor regardless of total score 3.
| Evaluation Criterion | Weight | Deal-Breaker Threshold |
|---|---|---|
| Account-level execution capacity | 25 | Per-location retainer model; cycle time over 21 days for a location page |
| Compliance-aware measurement architecture | 20 | No documented HIPAA-safe tracking; single attribution model for all decisions |
| Unit economics discipline | 15 | Refusal to commit to blended CAC and CAC:LTV targets in writing |
| Location-level data integration | 15 | Reporting latency above 72 hours; manual joins between platform data and bookings |
| Performance reporting against healthcare KPIs | 15 | No drill-down from portfolio to single location and provider |
| Team depth and AI execution capability | 10 | No named senior staff allocated; AI claims with no measurable CAC impact |
The weighting departs from conventional healthcare RFPs in two specific ways. Strategic approach and creative capability — categories that often carry 20 to 30 points combined in templates like the FV Hospital tender — are absorbed into execution capacity and measurement, where they have to prove themselves through shipped work rather than slide design 8. Total cost is not a separate line item; it is priced inside unit economics, because a retainer that produces a 40% higher blended CAC is not cheaper at any location count.
Deal-breaker thresholds matter as much as the weights. When every requirement is treated as equally critical, scoring collapses into a near-tie across finalists and the decision drifts back to chemistry 1. Naming three or four hard disqualifiers — measurement architecture, account-level pricing, reporting latency, written CAC commitments — forces vendors to either meet the bar or self-select out, which compresses the shortlist to operators who can actually run a 50-location portfolio. The scorecard then ranks survivors on capability depth rather than on which deck told the better story 2.
Unify Medical Marketing Across All Sites—See Coordinated Results at Scale
Connect with our team to explore AI-driven solutions proven to optimize content, PPC, and SEO across every location—without adding overhead or sacrificing performance.
Consolidation Economics: Per-Location Spend vs. Account-Level Programs
The economics of multi-site marketing bend in a specific direction past 25 locations, and the bend is what makes operating model the dominant variable in vendor selection. Per-location agency spend scales linearly with footprint. Coordination cost scales faster. Reporting cost scales faster still. Account-level programs flatten the second and third curves while holding the first roughly constant — which is why the comparison rarely turns on monthly retainer headlines.
The worksheet below frames the math in variables operators can populate with their own contracted retainer R. Patient acquisition cost is anchored to the sourced specialty range of $155 to $610, with a midpoint of $383 used for portfolio modeling, and lifetime value is held at the $10,000 to $20,000 band with a 1:3 CAC:LTV target as the threshold for healthy economics 4. The AI-execution column applies the sourced 30% blended CAC reduction that operators report when AI-driven production is implemented against the same channel mix 4.
| Footprint | Per-Location Retainer Model | Account-Level Program | Account-Level + AI Execution (-30% CAC) |
|---|---|---|---|
| 5 locations | 5R + light coordination overhead; CAC near midpoint $383 | 1R-equivalent + shared production; CAC near midpoint $383 | Blended CAC ~$268; CAC:LTV well inside 1:3 |
| 25 locations | 25R + non-linear coordination cost; cycle times stretch; blended CAC drifts above midpoint as execution slips 9 | 1R-equivalent + production scales sub-linearly; CAC holds near $383 | Blended CAC ~$268; portfolio LTV $10K–$20K preserves 1:3 ratio |
| 75 locations | 75R + coordination overhead dominates; reporting latency and missed deadlines compound; CAC pushes toward upper band | 1R-equivalent + marginal cost per added location is small; CAC stable | Blended CAC ~$268; ratio improves as LTV cohorts mature |
Two reading instructions matter. The retainer column is not cheaper at small footprints simply because 5R is a smaller number than the account-level fee; it is cheaper only if coordination overhead and CAC drift stay near zero, which holds at five locations and breaks somewhere before 25 9. And the AI-execution column is not a discount on the agency invoice. It is a reduction in blended CAC at the same or higher publishing volume, which is the line that actually shows up in the P&L. Sourced RFP guidance is consistent on the framing: lowest retainer rarely wins on long-term value, and contracts should be priced against ROI rather than headline fees 3. The operator question is not what the monthly invoice reads. It is what the cost per acquired patient reads at 25, 50, and 100 locations — and which operating model holds that number steady as the footprint grows.
 Potential cost savings from agencies using advanced AI technology: 30%
Potential cost savings from agencies using advanced AI technology: 30%
Centralized, Modular, or Account-Level: Matching Operating Model to Footprint
Three operating models compete for multi-site healthcare contracts, and each fails in a different place. Picking the right one is less about ideology than about footprint, service-line complexity, and how much in-house capability sits behind the agency relationship.
The centralized full-service agency concentrates strategy, creative, media, and reporting under one roof. It works at five to fifteen locations with a single service line, where consistency is the dominant problem and coordination cost is still tractable. It begins to break when service lines diverge or location count crosses the threshold where one account team can no longer hold the whole portfolio in working memory 9.
The modular specialist stack — separate vendors for SEO, paid media, content, and creative — buys depth in each channel and avoids single-vendor lock-in. The cost is integration burden, which the operator absorbs. Reporting reconciliation, brief alignment, and measurement consistency become internal jobs. The model fits operators with a strong in-house marketing ops function and 25 to 75 locations across multiple service lines, where channel depth matters more than coordination economy.
The account-level execution model treats the entire footprint as one program with shared production and location-specific outputs. Strategy, content, paid media, and reporting run against a single plan; the marginal cost of adding a location stays small. This is the model that holds together past 75 locations because execution capacity scales sub-linearly rather than headcount-for-headcount 9. The diligence question is whether the vendor can demonstrate account-level pricing, account-level reporting, and account-level approval workflows — not three separate retainers stitched together with a master services agreement.
Footprint and complexity decide the match. A 12-location single-specialty group with a strong brand voice is well-served by a centralized agency. A 40-location multi-specialty group with sophisticated internal marketing ops can run a modular stack. Anything past roughly 50 locations, or any portfolio adding three or more locations per quarter, should be scoring vendors on account-level execution architecture as the primary criterion 3.
Unify Multi-Site Medical Marketing with Automated Precision
Access a centralized platform to automate content, PPC, and backlink strategies across all locations—improving campaign speed, consistency, and measurable ROI for complex healthcare operations.
Contract Terms and Red Flags That Predict Failure
Contract language is where the selection rubric becomes enforceable, and where most multi-site agreements quietly default to terms that protect the vendor instead of the operator. The terms below are the ones that correlate with whether a relationship survives past year one without a renegotiation under duress.
Five clauses carry disproportionate weight. Performance triggers tied to blended CAC and CAC:LTV thresholds, with documented remediation if the portfolio drifts above the 1:3 healthy-economics line for two consecutive quarters 4. Account-level pricing rather than per-location retainers, so the marginal cost of opening location 26 or 51 does not reset the negotiation. Data ownership clauses that assign GA4 properties, ad accounts, call-tracking numbers, and location-page CMS access to the operator, not the agency. Reporting SLAs that fix dashboard latency at 72 hours or better and require drill-down to a single location and provider 5. And termination terms that allow exit for missed performance triggers without a full annual penalty, since the alternative is paying out a contract that has already stopped producing.
The red flags are equally specific. Refusal to commit to written CAC targets. Pricing that scales linearly with location count. Dashboards demonstrated only as static screenshots. Account teams introduced at pitch and replaced at kickoff. Measurement plans that propose one attribution model for every decision type 10. And the leading indicator that predicts the rest: a vendor that goes quiet during diligence. The 44% of practices that switch core vendors over unresponsiveness did not discover the problem after signing — the signal was visible in the sales cycle and overruled by chemistry 1. Contract terms are the operator's last chance to make the rubric stick.
Frequently Asked Questions
References
- 1.The EHR Selection Process: A 5-Step Vendor Evaluation Framework.
- 2.Everything You Need to Know About Healthcare RFPs.
- 3.RFP Evaluation Criteria: How to Score and Select the Right Vendor.
- 4.Patient Acquisition ROI: The Complete 2025 Guide to Measuring and Maximizing Healthcare Marketing Returns.
- 5.Top 26 Healthcare KPIs & Quality Metric Examples for 2026 Reporting.
- 6.Healthcare Marketing Trends In 2025 – 2026: Strategies Shaping the Industry.
- 7.15 Marketing Certifications That Can Help You Earn a Better Salary.
- 8.Request for Proposal (RFP) Tender on Marketing and Communication Services - FV Hospital.
- 9.Multi-Location Healthcare Marketing: How Organizations Manage Execution Across Locations.
- 10.P.A.C.E. Framework: Pharma Omnichannel Marketing Measurement.